“I’ve tried everyone else. I’m desperate.” Weekend, evening, call out fee, minimum charge, double time. Cash. It was a Trust-a-Trader call I couldn’t turn down.
I pulled into the drive of a red stone Victorian pile. Stone steps between armorial lions led to a recessed porch, flanked by columns, and an impressive oak panelled front door. Overshadowed by trees, a weak single and naked light bulb above the door was barely strong enough to cast my shadow onto the tiled entrance floor.
I was wondering whether to clap the huge brass tiger’s-head knocker or ring the bell, but before I could reach for either the sound of locks and chains being withdrawn made either superfluous. The door creaked slowly open, but only just enough for a fingerless gloved hand, with broken and stained nails, to grasp the edge and hold it steady. Half of a pale face, fringed by lank white hair, peered out, the piercing single eye scanning me up and down.
“Ah. I’m glad you called, we are let down so often”, the face said, and the door swung further back. “Come in, Mr…..Mr?
“Thank you”, I said, “James McIntyre. McIntyre Plumbing and Heating at your service. I take it you are Mrs Gill?”
The door opened fully to reveal the bent frame of a man. A grease stained, frayed and crumpled, frocked coat and collarless open-necked shirt, hung limply from his gaunt frame.
“I am not, as you can see, Mrs Gill” he said with a slight chuckle and not a sign of irritation.
“I am Arnold. You may call me Mr Arnold, as Mrs Gill does. I am her housekeeper and general factotum. She is unavailable at present, and it is me that called you. Please come down to the kitchen. It is where the problem is, and where all tradesmen are…..received.”
As I picked up my tool bag and followed Mr Arnold I had hardly noticed a sickle shaped scar, half hidden by his flowing hair, before we were off along a series of dark panelled passages to a narrow stair and down to the basement kitchen, the passages wreathed in must and disinfectant, and lined with stuffed mounted animal heads. His stride, off kilter though it was, was surprisingly lithe and hard to keep up with, but on the way I asked him,
“What is the problem, Mr Arnold?”.
“The drains are blocked again. I’ve had many plumbers to look at them, but it’s never fixed for long it, and they don’t come back to try again. We hope you will have more success.”
Mr Arnold showed me a massive, antiquated butler sink, full of something disgusting, and pointed me to a large grating in the stone-flagged floor, also brimming over. Outside the kitchen door a large manhole cover was similarly oozing at the edges, suggesting a very big problem.
“I think this needs clearing all the way down to the main drain, I’ll need my drain rods, and the pressure jetter for after I clear it” I said, but as I turned to go back to my van, Mr Arnold had apparently read my mind: he stood in my way, holding two bags full of rods.
“I thought you might need these to start with. Your colleagues always seem to, but then leave them behind. We have quite a collection if you need more. I will leave you to your work, Mr McIntyre, it’s time for me to take Mrs Gill her morning tea.”
It was painfully slow going and I was going to earn my money. Every now and again the end of the rod would grip on something solid, and then clear only to grip again, but eventually with a satisfying gurgle, and sucking noise, the residue from the sink and the grating disappeared. Result!
I was about to go up for the jetter when I heard footsteps on the stair and stood back. A thin faced elderly woman, her white hair pulled up tight in a bun, hobbled down.
“Mr McIntyre, I’m Mrs Gill. Mr Arnold suggested you might be needing some assistance. As you see, I am prepared.”
She had a plastic apron over her floral pinafore dress and was wearing pink rubber gloves.
“Indeed you are, Mrs Gill”, I said, “that’s kind of you but I’m almost finished. I just need to wash everything down and that’s me, done.”
“You won’t mind if I check everything, will you, Mr McIntyre. Mr Arnold dabbles with taxidermy, I expect you noticed his animal heads as you came in. He looks after me so well that I feel I have to allow him his hobby, but I do have such trouble with my drains.”
Something had been niggling at the back of my mind, and while the old woman ran the sink taps, set about inspecting the floor grating, and the manhole, I realised what it was. It was the way she and Mr Arnold referred to “me and we” as if they were interchangeable. A slip of the tongue perhaps, but when she bent over the floor grating, I saw a little scar peeping out at the edge of her bun. It couldn’t be, could it?
But then, apparently satisfied with my work, Mrs Gill pulled off a rubber glove to reveal a thin hand with broken stained fingernails, and my blood ran cold.
“Now, as to your fee, Mr McIntyre. I wonder if you are open to some sort of negotiation?” She almost caught me by surprise, by moving un-naturally quicky, and produced a long kitchen knife.
I struck out with a drain rod across the thrusting hand, put my shoulder into her chest, and knocked her backwards with enough force to allow me to sprint for the stairs. I didn’t know if I was being pursued, but I didn’t stop until I was, breathless, at my van. As I opened the driver’s door I thought I heard a chuckle, and then one of them call out,
Long, long, before the advent of social media, A.I. and “fake news”, people have been offered stories about secret societies, about politically motivated consipracy, about state sponsored manipulation of truth. Mainstream film and television drama, has consistently drawn on these ideas to create entertainment, that both feeds on but also fuels suspicion that what we see, and hear, is possible and therefore might just be true. In considering this, in the immediate aftermath of an alleged (and I’ll justify the use of this word later) assassination attempt on Donald Trump, I am reminded of the joke that “just because I’m paranoid it doesn’t mean they’re not out to get me”. The important word in the sentence is “they”, because the power of a conspiracy derives from people acting nefariously and in concert to achieve their aims.
Political and criminal assassination is commonplace across the world. In the “West”, today, and as far as we know, it is comparatively rare but if you are a Christian, you accept that Jesus of Nazareth fell victim to a conspiracy. If a student of ancient history, you will know that Julius Ceasar (and others) were murdered by conspirators, more recently India seems to be a particularly violent place https://en.wikipedia.org/wiki/List_of_assassinated_Indian_politicians and of course, in relatively recent times in America, there are two Kennedys, Dr Martin Luther King, and an attempt on the life of Ronald Reagan. Elsewhere, multiple suspicious deaths are laid at the door of the Russian Federation, and easily recalled.
It is noticeable that the person identified as the perpetrator in the attempted, and successful, assassinations in the US is suggested to be a sole actor, often portayed as an inadequate, under-achieving, “loner”, and this incident in Pennsylvania is initially going the same way. There will be an investigation (perhaps several) right now seems to be focussed on responsibility for the apparent failure to prevent the attempt, and what the motivations of Thomas Crooks (the alleged shooter) were, rather than the complete picture. However, there are legitimate questions which should not be glossed over in the rush to find someone to blame. I certainly have questions, especially in the belief that inquiries into earlier political murders in the USA have never really managed to shake off doubts about what happened – for example the death of JFK. Asking questions should not be immediately presumptive of a conspiracy theorist. After all, the authorities in the USA will also be asking questions. The important thing, in the pursuit of the truth, is that no questions should be left unasked because they are thought to be outlandish.
So, my questions are these:
Donald Trump was over an hour late in arriving at his rally. Within minutes of him taking to the stage a shot, or shots, were fired. It means that if Matthew Crooks was the, and only, shooter he must have been in position for more than an hour ahead of him firing. How was that possible? He did not appear to fire “from cover”, as a sniper normally would, and he did not appear to be camouflaged in any way.
The audio track of the attack appears to have several shots: an initial two, followed by a short volley – perhaps 6 in total. Were they all fired by Crooks, that is to say were any of them being fired by Secret Service snipers (SSS) who were credited with killing him? If the SSS did shoot Crooks so promptly, as has been suggested, how did they manage that when, by all accounts, Crooks had been undetected (unseen) by them before he fired? If they were all fired by Crooks, what was he shooting at after Trump hit the ground? As well as Trump, two others have been badly wounded, and another died. I assume that, if recovered intact, the bullets could be matched to Crooks’s gun and no other?
An extraordinary photograph has appeared which seems to show a bullet passing behind Donald Trump, level with his head – perhaps the bullet which is alleged to have hit his ear. The path of this bullet, if genuine, seems horizontal, yet the position of Crooks was elevated above the stage – shouldn’t the path of the bullet have been downwards?
It initially appeared that Crooks was not an expert marksman – it was alleged that his request to join a college shooting club was rejected, but he was in a local gun club. Certainly, at that distance, an expert marksman should not have missed, especially with prominent windage markers (flags) available. Military grade snipers regularly ‘kill’ at distances in excess of 2000 metres, so a shot measured in hundreds of feet should be easy.
Finally, for now, apparently Crooks had no I.D. on him because it is said his body had to be identified from DNA, and it appears to have been done very quickly. How long does it take to retrieve an uncontaminated sample, from a body on a roof, for DNA sequencing? Having done that, how long does it take to run the test? Having done that, against what record (database) of a DNA profile was it matched? I don’t think Crooks had a criminal record, so his DNA should not have been in “the system”but, perhaps thay actually used fingerprints, which might have been in a database from a driver’s licence or gun licence application?
So, to return to my initial use of the word “alleged”. As things stand the general public doesn’t really know what happened, but we are beginning to see what the consequences of this event may be for the 2024 US Presidential Election and, on the basis of the evidence so far, Donald Trunp now looks likely to be a “Shoo-in”.
In my blog immediately before the election, which Labour won by a “landslide”, I spoke about the Conservative’s inability to grasp that, no matter their record, their positioning and electoral “offers”, they just didn’t ‘get it’. I suggested that the electorate had a sort of ‘Conservative fatigue’, that after 14 years of Conservative governments, the electorate just wanted something different – a change.
In the aftermath, and I write this only a week after the election, several former Conservative ministers, some that had retained their seats, have already spoken about the reasons for their defeat. Of course there is already jockeying for position, by those with political ambition to rise through the Conservative ranks, and even to leadership.
However, in their statements, they have demonstrated just how out of touch they really have been. None of them (that I have heard) have looked inwards at their failures, at their record, but instead have pointed to a failure to “deliver”. What they seem to have missed is that, had they “delivered” on their (most recent) manifesto promises, they would still have presided over a deeply divided, polarised, and unequal country which was ready for a change.
It is typical displacement behaviour to point to external influences (like Covid, like the war in Ukraine, like Gaza) rather than address uncomfortable, even painful, truths closer to home. None of them, so far, have called a spade an ‘effing shovel’ and said sleazy, lying, party-over-country, and incompetent politics has undone them. If they don’t have a “road to Damascus” moment, then they are doomed to repeat the same mistakes when next they form an administration, and we are doomed to suffer it all over again.
The televised head-to-head “debate” between the UK’s incumbent PM, Rishi Sunak (Conservative) and Keir Starmer (leader of the Labour party) had plenty of sound and fury but little illumination and it gave this elector, who had already cast a vote by post, no reason to regret his choice.
The UK is a parliamentary democracy and the UK Election is NOT a Presidential Election. While leaders of our political parties are the face of any government they lead, they lead a cabinet team – for the time being – because our Prime Minister does not have the wide executive power of a president. I say “for the time being” because, in recent years, there have been mulitple changes of Prime Minister, during the period of a Conservative Government, leaders who nobody but a privileged few actually voted into office.
The debate, if you can call it that, appeared to give us the electoral choice between a decent blancmange and a bullying wide-boy. However, it is what, and who, is behind these two figureheads that really matters. Sadly, for this voter, there is apparently little to choose between the Conservatives and Labour ‘offers’, as the parties have fought for the same middle ground votes. But what is in the DNA of each party, and their MPs that, if elected, will define their respective approaches to issues of domestic and international politics?
The UK has had 14 years of Conservative government, and (I would argue) ever since Theresa May was shafted by her own party it has been a party increasingly driven by opportunism, by the desire to promote individual advantage and wealth accumulation at the expense of public services – which is, after all, what Conservatism is about. In the same period the Labour party, as distinct from the Labour movement, has tried to reposition itself as Tory-light after a brief flirtation with socialism (under the leadership of Jeremy Corbyn) proved electorally disastrous.
What I think the Conservatives appear to not grasp is that, no matter the rights or wrongs of their respective propositions, after 14 years of them people just want a change: there is a natural lifespan to governments and we are at the end of this one.
Nevertheless I am depressed that there has been little discussion about, or review of, the policies being pursued and their failures, over that 14 year period. Extraordinarily, except amongst the minor parties, there has been no mention of the massive act of national self-harm known as Brexit. Quite apart from the claimed economic benefits, which have not (yet) materialised, a major (and I would argue the main) reason why the 52% of pro-Brexit votes were cast was on the single issue of immigration – “getting our country back”. This has signally failed to happen and is still an electoral issue, now being exploited by the right wing Reform Party.
The national finances are in debt and, ignoring the shambolic Liz Truss mini-budget that crashed the already weakend economy, Sunak points to the unanticipated financial burden of the war in Ukraine and, especially, the Covid pandemic. (You can read more about my experience of, and thoughts about, Covid here http://www.harrygoldjazz.com/category/covid-19/ ) The present PM was, at the time of the Covid outbreak, Chancellor of the Exchequer and provided support through the so-called furlough scheme. Credit where it is due, it was essential. It stopped the country being bankrupted, and saved millions of jobs. The development of a vaccine and its (continuing) roll-out was also major achievement, but the debt burden of this multi-billion support is now being carried by us all (except those who have made a packet out of PPE contracts!) and what nobody in mainstream politics is saying is that it was made worse than it needed to be by 3 things, which were, and are, under government control:
a lack of preparedness for a pandemic, despite a warning to that effect in 2016 which said amongst other things that stocks of PPE were inadequate.
being slow to respond to the developing threat, at a time when a week or two’s delayed action was critical, and then late adoption (and enforcement) of simple infection control measures like face masks and social distancing. Partygate and Barnard Castle anyone…?
an unbalanced economy.
In the UK we are economically dependent on services: ever since the Thatcher era the UK has been increasingly dependent on selling, and not making, ‘stuff’. Our taxation ‘take’, and therefore ability to deliver public spending programmes, is overly dependent on us ‘consuming’. The furlough scheme was in large part directed to supporting service industry of various kinds, and by directly encouraging us to spend what little money we had e.g. the “eat out to help out” scheme. Repeated attempts to relax ‘lock downs’ and social distancing measures to stimulate the economy, predictably promoted resurgence of the virus and damaging consequences. You can see my commentary on this here http://www.harrygoldjazz.com/2020/06/19/shop-til-you-drop/
I would argue that rebalancing the economy should be a lesson from Covid, a priority for any incoming government. In a planet facing the existential threat of climate change I would also claim that reining in consumerism would be good for the planet too!
My last post in this category was in 2017, 7 years ago, but I am moved to draw it to a close with an interesting, and I hope illuminating, footnote.
In 2017 I was still ruminating on the nature of residual symptoms, on the possibility that they might be long-term effects of Lyme disease, or might even be persistent infection. I was ‘negotiating’ with my GPs and hospital consultants about it, and struggling against their reluctance to admit that Lyme could persist after treatment and, in my case, massive and prolonged antibiotic therapy.
In 2018 I suffered a fall which resulted in a bad leg injury. The consequence of an emergency operation, and inadequate treatment, was a serious infection and emergency admission to hospital for another operation. After 4 days of intravenous antibiotics my residual symptoms suddenly disappeared and have not returned. Clearly, in spite of medical reluctance about ongoing Lyme, something was going on and I shall always believe it was Lyme disease.
(This story was prompted by a friend who told me of a family cat who had joined her in bed early one morning – the cat was called Dave, but his full name, apparently, was Captain Davy McBoing Boing)
“Shiver me timberrrrs!”
A booming salt-caked gruff voice bounced off the pitch pine panels that lined the cabin walls, rattling pipes in a silver mounted pipe rack on the mantel.
“Avast there ye creepy landlubbers”! “Stand to and prepare to haul away, for we sail for the Spanish Main at midnight”.
Captain Peregrine McHardy threw back his head, ran his fingers through his long greying hair, tweaked his even longer yellowing, and tobacco stained, beard. Then, “Step thud Step thud”, he stomped across the deck on his wooden leg to the leeward rail of his barquentine, The Dark Lady, raised a telescope to his one good eye and purred with satisfaction at the view.
The view was across the neatly clipped lawns of the Cedars, a Nursing Home for retired seafarers or their dependants, not the quayside of a Caribbean Island, but did nothing to penetrate the illusion. The Dark Lady rode easily on the calm waters of Captain McHardy’s imagination.
“Did you hear Mr McHardy this afternoon, Matron, he was really away with the fairies at teatime? I’m afraid he’s getting worse.”
Matron Jeanne sighed, then shifted her considerable weight uneasily, her heavily carved antique chair squeaked in protest on its four brass castors.
“I agree Marianne, but The Captain’s condition is benign, so far at least. You haven’t been with us long, but the duty doctor examined him only last week and, apart from his eccentricity, said he’s harmless enough and pretty fit for a 99 year old, even with a leg missing. As long as he stays fit, and his fees keep being paid, there’s no harm and The Cedars will cope. We’ll keep him under review.”
“Actually, I’ve been thinking that we might get him a pet, something to focus on that’s real, not imaginary. Since the parrot we used to have in the residents’ lounge died he’s seemed a bit sadder somehow. The local Cats Protection down the road have lots of demand for kittens, especially round Christmas, but they’ve put round a flyer about a poor old ginger tom called Dave that they can’t find a home for. Partly it’s because of his age, but also he only has three legs and lost an eye – results of a hit and run – so he wouldn’t be a wanderer and he might be good for the home more generally. What do you think?”
Three weeks later and preparations for the Cedar’s Christmas party were almost complete, but it was going to be a challenge to coax all the residents out of their rooms. The prospect of two hours of carols, and sing-along show tunes, led by Leonard Pomfrey, his ‘swinging’ electric organ, and his glamourous assistant Mabel, were disincentive enough but, the idea of pushing peas and carrots round the gravy for their old relative was more than many sons, daughters, nieces, or nephews could contemplate. For the most part they had politely declined the invitation, citing a variety of reasons, some more convincing than others, preferring instead to visit before their own home celebrations, or rushing off to an airport to escape entirely in the warmth of a Spanish or Portuguese villa. And so the party would lack the joie de vivre engendered by fresh conversation and new faces but, as well as delivery of frozen turkey-filled vol-au-vents, individual pavlovas, cubes of pre-cooked roasted potato and, of course, peas and carrots, The Cedars had taken possession of Dave, as had Peregrine McHardy, or perhaps it was the other way around.
Peregrine McHardy had elaborated Dave’s name, and given him the honorary rank of Captain: Dave had become, to McHardy at least, Captain Davy McBoing Boing. McHardy had tried at first to appoint him as his First Lieutenant, “Number One” to his own command, but Dave would apparently have none of that as he would not respond to any call other than “Captain”. As for Davy, well it seemed more piratical than Dave, and right for his one-eyed confederate whose scars gave him the caste mark of a buccaneer.
He had added the patronymic ‘Mc’, to align with his own Mc – though truly that was also a fiction because Peregrine’s real name was Hardy. He’d felt the need to differentiate himself from Nelson’s Captain Hardy, because being a Hardy had been the source of recurrent and irritating “kiss me” jokes throughout his own maritime career.
Quite where the “Boing Boing” part came from he could, or would, not explain. Instead, he left it to speculation, with a knowing wink from his good eye, saying “That’s for me to know and you to find out”, with more than a hint that it might be something ribald or risqué in some Caribbean patois. Within two weeks of his arrival at The Cedars the two Captains would stroll the garden decking outside McHardy’s room, between them their uneven gait giving an uncanny impression of a ship in motion. At other times they could be seen sitting side by side, at the railing, apparently reminiscing about past adventures or sharing more intimate moments as Captain Davy rubbed his ginger head through McHardy’s beard.
Once established at The Cedars, and trusted almost as a member of staff, Captain Davy was allowed to walk the corridors, visiting the other residents room by room dispensing, not medication but something just as powerful and though there was never any doubt about McHardy’s primacy, Captain Davy’s independence was also never in doubt. He went where he pleased, when he pleased, but also where he was needed.
In the days between Christmas and New Year the Cedars drifted, becalmed in a kind of social doldrum. Not much happened, no-one much visited, even the doctor stayed away, and it was a time that Matron Jeanne, Marianne, and her other colleagues always valued as an opportunity to review, but this year there was something unusual to discuss. Stocks of some medications were not declining at a normal rate. Of course, that might be a natural cyclical phenomenon. As residents came and went the need for medication varied, but there had been a decline in the need for anti-depressants, for sleeping pills and so on. Even call for routine medications for Parkinsons and Alzheimer’s seemed to have reduced. The doctor’s surgery had noticed that the regular dispensing of repeat prescriptions had dipped and, concerned, had enquired as to why.
It was Marianne that spoke up.
“I know this sounds silly, Jeanne, but I think it began when Captain Davy came to live here. I know we got him for Captain McHardy, and that’s worked, he’s definitely happier, but all the residents love him. We’ve all noticed that when we do the blood pressure checks, especially after Dave has done his rounds, most of the readings are down and they are staying down. Not much, but they are down. We’ve also noticed the residents are sleeping better, some of them even grumble when we wake them up for breakfast!
Meanwhile Captain Peregrine McHardy had begun to leave his room more often too, and sometimes would patrol the corridors and lounge in company with Captain Davy. He would stomp around, and could be heard issuing orders to Captain Davy, for example to “batten down the hatches” or “reef in the sails”, when the weather forecast was bad.
On Captain McHardy’s 100th birthday he was found on the deck, in full dress uniform, surrounded by photographs of some of his ships. He had cast off for his final voyage. Captain Davy sat by his side, quietly mewing for orders. He attended the funeral, along with Matron Jeanne, Marianne and someone from the Seamans Mission, but though Captain Davy returned to The Cedars he didn’t stay, and one night he just slipped away. But the gifts he had brought to The Cedars did stay, and a new cat came from the shelter, a female, that they named Lady Mary Killigrew. As the years passed other cats came and went, but a tradition had been started. Out of respect to the two Captains who began it, but especially Captain Davy McBoing Boing, however many legs or eyes they had, they were always named after pirates.
Even with family, with social connections, people can feel alone at times. Even if they aren’t alone they can feel they are. They may or may not feel lonely, which is a different thing from being alone, in fact people who are not alone can still feel lonely; a feeling of emptiness that is not unlike that of hunger. It feels like hunger because that is what it is.
The media, television companies especially, even more so at Christmas, focus on joy, on excitement, on being not alone, satisfying a need for something which is sublimated into a need for new, for bigger, for better and the commercialism of the modern world is only too happy to exploit it.
The collateral damage, the human casualties, we probably don’t think about for a few days at least – if we ever did. Perhaps, because they can’t avail themselves of the balm of excess, we maybe feel guilty about them: fortunate to not be them and uncomfortable about it. When you don’t even have a roof over your head, or food to eat, being made to yearn for Jimmy Choo or Gucci is at best cruel, but what might we lack and may have in common with them?
The reality for many is that the need, this yearning, is for something deeper. Alone this year and binge watching a continuous stream of (especially American) made-for Christmas movies, I’ve realised that, formulaic though they are, they touch on common themes.
They all seem to offer hope: hope of redemption, or simply hope for a kinder future. They seem to value connectedness to values we may have lost, the importance of giving not taking, turning our backs on opportunism, and especially the need for, and to find, love. Oddly, one of the most iconic (to the ‘west’) and much loved of modern Christmas stories, Dickens’s “A Christmas Carol”, does not have the pursuit of love as a central theme, although the loss of the youthful love of his sweetheart because of Scrooge’s greed and ambition is an issue. Other seasonal filmic offers are similar: “It’s a Wonderful Life”, for example, focusses on the love of man, not romantic love.
Christmas is an important religious festival for practising and devout Christians. For the rest, non-practising but perhaps brought up in the context of a Christian tradition, acknowledgement of something missing in our spiritual lives is circumvented by willing acceptance of, even faith in, something miraculous or supernatural but religiously ‘safer’: fairies, angels and Father Christmas.
Faith can be defined as a belief in something, or someone, on the basis of conviction rather than empirical proof: evidence. All the world’s religions are founded on faith (though some adherents of relgions would say there is proof for their particular faith. So, whatever your faith, or none, if you are alone at Christmas, and feeling a gnawing hunger, try reaching for something less tangible, but maybe ultimately more filling, than food or material possessions.
I wrote this a few days after the brutal Hamas incursion into Israel. It’s extraordinary how things have changed in the global context. Assad has gone from Syria. Trump is in power in the USA and, being a brazen property developer, says he will “take over Gaza” and relocate Palestinians to do it, creating a multi-ethnic “Riviera” development. Between them, Israel and America should pay massive reparations for destroying Gaza, not profit from it.
On 7th October 2023 a complex, sophisticated, and multi-modal assault was launched on southern Israel by Hammas, a so-called Palestinian ‘militant’ organisation, from within Gaza. There have been minor exchanges of fire with Hezbollah in Lebanon, another so-called ‘militant’ organisation, in the north of Israel. It has, so far, resulted in thousands of deaths and injuries, in both Israel and Gaza, the kidnapping of Israeli men women and children as hostages, and the retaliatory arrest and incarceration without trial of thousands of Palestinians within Israel itself and the Israeli-occupied territories. It has led me to wonder what (and who) might be behind it?
Some of the Israeli civilian casualties, including women and children, were slaughtered, wholesale, in a bestial outpouring of hatred and anger, and rightly condemned around the world. As I write this, the Israeli military is pounding Gaza into rubble, also indiscriminately killing civilians, and in an extended act of revenge and reprisal Gaza has been effectively cut off from water, electricity, food and medical supplies. Though the United Nations Organisation, and other diplomatic channels, describe this as a war crime and a breach of international law, in general the world response to Israeli actions has, so far, been notably muted, even presented as Israel’s right to “self defence”. If evidence were required, though, of a beligerent attitude underlying the Israeli posture, a representative of the Israeli Defence Force (IDF) has been quoted as saying “”The IDF is capable of operating anywhere required and will strike any force that endangers Israelis. We will do this in any place (my italics) where it may be required.” We already know that forces from Israel have, for years, operated in Iran, Yemen, Syria, Jordan and so on, reaching out in pre-emptive acts of “self defence”.
There was surprise that the Israeli intelligence services, acknowledged to be amongst the most effective in the world, appeared to have been caught napping: they didn’t see it coming. Or did they? Reports emerged that Egyptian sources warned of an imminent attack three days before it started. Other reports, from Israeli reservists, warned of unusual military activity along the border for weeks before, reports that appear to have been ignored. An Israeli military spokesman referred to the shock as being like that in the US caused by 9/11 and Pearl Harbour, so it is ironic that similar reports sufaced of ‘ignored’ warnings after Pearl Harbour. Pearl Harbour brought the US into WW2, from sitting on the sidelines, and ultimately led to victory for the Allies. Some within Israel might have thought the price paid, as at Pearl Harbour, was worth the sacrifice made, by ignoring warnings. I have no doubt there are many in Israel who would dearly love to destroy the Palestinians as much as there are some Palestinians would like to destroy Israelis and the state of Israel. There can be no doubt that the Hamas attack on 7 October gave Israel a cast iron excuse to do just that. Did the hard-line, right wing, nationalist Israeli government secretly think that allowing the incursion that resulted in the deaths of 1200 citizens and abduction of 250 was a price worth paying? Whoever masterminded the attack, Hamas and their fellow travellers could not possibly have expected to destroy Israel by their actions on 7 October, but may have thought, strategically, the consequences of the inevitable Israeli reaction might ignite a regional reaction that would achive that for them.
It is a truism that nothing overcomes internal divisons quicker than an external threat and, until this latest conflict happened, Israel was deeply divided with unease, even in the military, of the direction of travel of the right wing coalition government. The Prime Minister, Benjamin Netanyahu, is under attack for pressing through reforms to the judiciary which are intended to limit the freedom of the courts. These reforms are so divisive within Israel, so anti-democratic, that some army reservists (on which the Israeli military depends) had threatened to not turn up if they are called. Mr Netanyahu is also under indictment for bribery, corruption and fraud, so this is a welcome distraction for him, but there are many, including at all levels of Israeli society, who are worried about the seemingly inexorable progress towards a theocracitic state: the conflation of Judaic law and civil law. An inevitable consequence of this is that criticism of the state of Israel, or the actions of its governments, is labelled as “anti-Semitic”. Whatever one thinks about the former leader of the UK Labour Party, Jeremy Corbyn, his inability to counter a label of being anti-semitic because of his overt support for the cause of Palestine, and his criticism of the state of Israel, cost him his job, cost Labour the next General Election and precipitated a change in Labour Party policy. All Jews, and even people with some Jewish heritage, know that anti-semitism, in thought and action, is real and ever-present, but today’s conflict seems to have precipitated an eruption of both in the UK. However, in the second world war, and ever since in the re-telling of its history, the same conflation of Germans and Germany with Nazis and Nazism took place – and continues to this day. We have seen what happens when the secular and democratic life of a nation is overtaken and suppressed by an ideology or theocracy: Afghanistan and Iran are two examples of the latter, with Saudi Arabia not far behind, and the active inclusion of the Russian Orthodox Church in Russian politics is yet another example.
Not all Israelis are Jews. Not all Israeli Jews are Zionists, not all Arabs are Muslims, not all Arab Muslims are fanatically anti-semitic or anti-Zionist. It is not beyond the bounds of possibilty that the forces from Gaza that inflicted such grievous and bestial harm are not even from Hammas’s own cadres, but from groups such as Isis/Islamic Jihad acting as proxies. At least 4 distinct groups (so-called Brigades) of fighters, representing different factions within Gaza, have been identified as having taken part. It is very muddy, too muddy for broad brushes. The term “Palestinians” is used as if they were a homogenous people from an identifiable land/country. They are not. They are a disparate multi-ethnic population, 75% of whom are regarded as refugees, and many of them are living in refugee “camps”. Not all so-called Palestinians support Hammas or Hezbollah, or indeed any of the many political or neo-political groups that seek to represent them such as The Palestine Liberation Organisation, Fatah, The Palestinian Authority and so on, but it suits some agendas, including those of a lazy and compliant world press, to lump everyone under one umbrella and paint them as “Good or Evil”. There is no room on the front pages of the tabloid press for nuanced reporting. The BBC, to its credit, published an early piece by veteran reporter John Simpson explaining why the BBC steadfastly refuses to label Hammas as “Terrorists”. Even long-term Middle East reporter Jeremy Bowen seemed to have been choosing his words very carefully and it took the BBC a week to start more in-depth objective and contextual analysis of the wider and historic causes of Middle East conflict. At first I only found a BBC Radio 4 production in the series “Briefing Room”, broadcast on 12th October, which was followed by a daily podcast, but the daily output on mainsteam TV (especially) was, in my opinion, ‘soft edged’.
Taking a step back, to allow a wider perspective, one wonders who, ultimately, will be the beneficiaries of a new Middle-East war? For example, in the global context, it undoubtedly suits Vladimir Putin to have the west’s attention taken away from Ukraine, it also suits him to have munitions earmarked for Ukraine, only a few days before reported to be scarce, to be diverted to support Israel. I would venture to speculate that this war also suits some other Middle-East nations. Assad’s Syria, for example, is a bedfellow of Russia and Putin and out of the rubble of their own civil war would like again to be a key player in the Middle East. Iran, for example, a rigidly theocratic state implacably opposed to the ‘West’ and the West’s client states like Israel, also has regional ambitions. There are increasing indications of what may be attempts by either “side” to provoke an extension of the conflict into Lebanon. Hezbollah, based there, is a massively well armed and well trained organisation: a wholly different order of opponent of Israel from Hammas. Since October 2023 Hezbollah has been firing a few rockets into northern Israel, allegedly in support of Hammas. Israel responds by firing artillery, some loaded with illegal white phosphorous, and mounted air strikes into Lebanon in response. Israel has claimed their forces have intercepted (i.e. shot down) drones flying from their territory, including from Yemen. There is also a largely unreported conflict on the so-called West Bank, where heavily armed illegal Israeli settlers, with the tacit (or actual) encouragement of the Israeli government, are intensifying ongoing raids into Palestinian/Arab lands and forcibly evicting the legal residents. It all feels, to me, like a deliberate series of provocations intended to justify a wider war – and I wonder, to whose agenda?
I would argue, it is not completely ridiculous to ask whether the backers of both main actors in this war, Israel and “the Palestinians”, are being manipulated by others to create a situation that results in changes to the intractable conflict, for their own regional ambitions, and this is why the international response has been muted. While people on all sides are dying, apart from some appeals for restraint, the major governments are waiting to see how this plays to their overall strategy for the region. When considering such an apparently ludicrous and machiavelian idea it is helpful to review how, and why, it got this way.
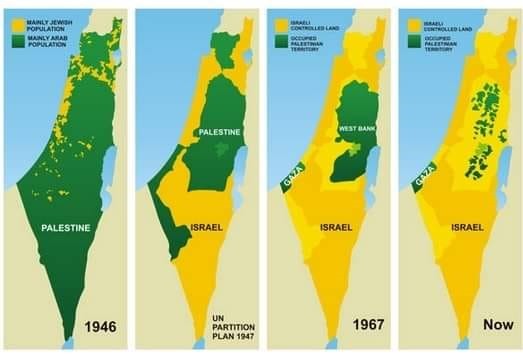
The creation of the state of Israel, a homeland for Jews, in the guilt-ridden aftermath of the second world war was (I contend) at best badly mishandled, at worst a mistake. The 1917 Balfour Declaration led to the creation of a national homeland for Jews, and this Wikipedia article bears some study. https://en.wikipedia.org/wiki/Balfour_Declaration. Critically it did not propose that a state of Israel would be established in all of the territory then known as Palestine, and it specifically said that the rights of the Palestinians, who then represented the vast majority of the population there, should be protected. Understandable in the recognition of the Nazi Holocaust (whose ghost has been raised by the present Israeli government), and the historic and historical oppression of Jews everywhere, the way in which it then happened by the forced appropriation of lands belonging to Palestinian Arabs planted the seeds of the present atrocities. Britain’s mandated control of Palestine was wrested from it by armed struggle with who we would now call Israelis but, at the time, we called terrorists: Irgun and, often known pejoratively as the Stern Gang, “Lehi”. Lehi was a Zionist paramilitary militant organization. Large swathes of what we now call the Middle East was colonised, mainly by Great Britain, France, Germany and Turkey, the major protagonists in the First World War, and the ‘redistribution’ of colonial ‘spoils’ after that war set the stage for what we now see. See this link for some more information: https://www.nam.ac.uk/explore/conflict-Palestine
There are elements within the Israeli establishment, and having influence over the establishment, that I believe would like to ethnically “cleanse”, and militarily sanitise, Gaza of Arabs: to replace the population with Israelis. Not many will say so openly, but for some Israelis the ideal solution would be to push the Gazan Palestinians into the sea, or over the border into Egypt. I would go further and say Gaza bears ironic and ugly comparison with the Jewish ghettos of eastern europe, and the inevitable consequences of that in the so-called holocaust. Gaza has become a kind of concentration camp, and the suggested forced ‘evacuation’ of the populace for their own safety, is just another kind of Pogrom which should resonate with some Israeli Jews. The modern political and military rationale is that Gaza is an open sore threatening Israel. The political and economic rationale is that Israeli occupation and control of Gaza gives Israel uninterupted access to the Mediterranean from the border with Egypt in the south to Lebanon in the north.
And if Israel did achieve a completely unified border, and contiguous land mass, what then? Would its historical, almost genetic, insecurity be assuaged? What, for example, of it’s borders with Lebanon, Jordan and Syria, which have already been ‘adjusted’ by occupation of the Jordanian ‘West Bank’ and the Syrian Golan Heights? With both sides seemingly held hostage by extremists, and with a Russian backed Assad in charge of Syria, what new flash points might there be? What of the land annexed by armed Israeli settlements, what of Jerusalem? Are these not just future Gazas which, in time, Israel would claim need to be ‘dealt with’ in the name of “self defence” and its national security?
With the increasing likelihood of a right-wing Republican government, and President, in the United States, one historically inward looking, will Israel be hoping for a ‘free hand’ over the next 4 or even 8 years? Will the election of an, apparently, more moderate leader in Iran impact on Hezbollah? We shall see.